

This is a free online resource, managed by the Institute for Behavior and Health, for substance use prevention coalitions, student prevention groups and clubs, and anyone interested in having an impact on youth substance use. It is important that the goal of youth prevention be articulated as a health standard – One Choice: no use of any alcohol, nicotine, marijuana, or other drugs for reasons of health.
One Choice celebrates the fact that an increasing number of young people are making the healthy decision to avoid substance use, and shines a light on that trend.
One Choice is a prevention message, not a program. This Toolkit includes guidance to help you incorporate the One Choice message into existing prevention programs or new prevention initiatives.
It provides scientific research on substance use and the developing brain, and aims to encourage student leadership and active involvement in prevention efforts. One Choice offers a platform for students who are making the decision to be substance-free to share that choice with their peers. Developed by the Institute for Behavior and Health (IBH) and Rye Action for Children and Teens Community Coalition (RyeACT), with input from a student advisory board, the Toolkit is organized around three essential facts that support the One Choice prevention message:

Fact #1
The developing brain is uniquely vulnerable to substance use
Fact #2
All teen substance use is related
Fact #3
There are a growing number of teens choosing not to use any alcohol, nicotine, marijuana or other drugs

Why One Choice?
Young people who choose to use substances, even if rarely, face many more choices: which drugs, with whom, how often, how much? A growing number of youth across the country are making the One Choice not to use any substances, a choice that is grounded in health. The science is compelling:

This Toolkit is not a step-by-step instruction manual for a program, but rather a resource that will provide you with information, guidance, and materials to create a strong drug use prevention message that can be shared with students and parents in your community. Featuring tips, ideas, and pre-made materials, the goal is to make your life easier as you incorporate the One Choice message into your own programming.
Over time, we hope to build a One Choice Community (OCC) online platform so prevention groups can share their successes, innovative ideas, and enthusiasm for student prevention with one another. Organizations will have the opportunity to have their work featured on the OneChoicePrevention.org website. This Toolkit will be updated periodically with new data, research, and insights from prevention organizations.
Does your prevention program…?
There is no ‘right’ way to use the One Choice Toolkit!
It is designed to be adapted to best fit the needs of your organization. We believe you’ll find the information helpful to you no matter what constraints your organization is under. We hope you will take the time to examine your current programming and observe how it aligns with the suggestions found in the Toolkit and share your experiences with the One Choice Community.

a note on language:
The terms youth, teens, young people, young adults, and students are used interchangeably
Youth should be part of the conversation about what terms they prefer in your community.
substances, drugs, and substance use
Refers to all nonmedical use of chemicals that stimulate the reward mechanism in the human brain, including alcohol, nicotine, marijuana, and opioids, among others.
substance use disorder
Refers to the brain disease of addiction. A substance use disorder used to be categorized as either “substance abuse” or “substance dependence” but now substance use disorders are categorized as “mild”, “moderate” or “severe.” (DSM-V) When an individual has a substance use disorder, their brain reward system has been altered. Substances hijack this brain mechanism producing pleasure without a biological benefit. Over time, with repeated use, they trick the brain into prioritizing substance use despite negative consequences of that use. All around the world, substances that are legal for adults -- alcohol, nicotine, and now in some places, marijuana -- are legally prohibited for youth because of the unique vulnerability of young, developing brains to these addictive chemicals.
Binge alcohol use
Defined as more than 5 drinks in one sitting.
Heavy alcohol use
Defined as binge drinking more than five times in one month.
Marijuana
Describes the cannabis sativa plant. THC (delta-9-tetrahydrocannabinol) is the primary component that produces psychoactive effects.
.

Brain Development
Children, young adults, and those that care about them, need to know that the developing brain is at a heightened risk for substance use disorders. While we tend to associate brain development with young children, this developmental period actually lasts into the mid-20s.
Adolescence is the time in which people tend to take more risks and seek high pleasure activities, including substance use. Early initiation of substance use can have lasting adverse effects on brain function. By educating students and young people on the unique qualities of the developing brain, they can make informed decisions about their own health. Non-use is the safest option for youth health -- a message that is supported by science and articulated by the American Academy of Pediatrics.

People under the age of 25 are at a heightened risk for substance use problems, including addiction.
Substance use in adolescence can change brain functioning and some changes may continue even after youth have stopped using.


Provide young people with the information they need to make One Choice for themselves. This message promotes teen self-care and autonomy.
Substance use in adolescence is not a moral issue; it is a health issue.

What you should know
and how to share it with others

The Fact:
The brain continues to develop into the mid-20s.
What this means
This series of brain images shows how changes occur from ages 12 to 20: from the least developed areas of the brain (depicted in red, yellow, and light green) to the more developed areas (blue and purple). Only the very small areas of dark purple are fully developed. The brain is fully developed around age 25.
This means that throughout high school and young adulthood, students’ brains are changing and developing. While exciting, it means that the developing brain is uniquely vulnerable to anything that negatively affects it. This is why there is so much emphasis on wearing bike helmets and following concussion protocols for this age group -- and why extending substance use prevention messages into early adulthood is so important.

Start a conversation!
Ask students to identify their own brain on the above graphic from Gogtay, et al. Where on the graphic are their siblings? How are they different?
Ask youth to identify their reason(s) to protect their brain -- what do they want to achieve? What do they care about that could be impacted by substance use? Am I a student? Am I a friend? Am I part of a family? Am I a problem solver? Am I an activist? Am I an athlete? Am I a teammate? Am I an artist? Am I a musician?
Ideas for sharing with others:
This is an opportunity to focus on health. Making One Choice to protect the developing brain from substance use is analogous to making other healthy choices like:
Wear a bicycle helmet
Use a seat belt
Exercise regularly
Eat healthy foods
Get enough sleep


The Fact:
9 in 10 adults with substance use disorders began smoking, drinking, or using other drugs before age 18.
What this means:
Substance use disorders are pediatric-onset diseases, and the risk of developing a substance use disorder is much greater for individuals that start using any substance before the age of 18.

Ideas for sharing with others:
This is a fact that is best stated simply. Hearing this number, “9 in 10” immediately makes people pause.
Be open. Be honest. Avoid statements like, “If you start smoking pot your life will go down the drain and you will die.” Our students are smart and have life experience. They have friends, neighbors, and/or parents that have achieved high levels of success despite a history of substance use.
Remember that public health recommendations are driven by population-level health outcomes, not individual experiences.

What this means:
Graph 1 - alcohol
The graph at left shows that adults who began drinking before age 21 were much more likely to have an alcohol use disorder in their lifetime than those who delayed drinking until age 21 or later. Among adults who drank alcohol at age 13 or earlier, 47% had an alcohol use disorder. Only 9% of adults in this study who had their first drink after the age of 21 had an alcohol use disorder.
Graph 2 - Marijuana
The graph at right shows data from a smaller study of individuals who recently initiated marijuana use (within 2 years) and had marijuana use disorder. For those who initiated at age 13, the rate of marijuana use disorder was 17%. By contrast, for those who initiated at age 21 or older, the rate of marijuana use disorder was 4%.
GRAPHs 3 & 4 - NONMEDICAL USE OF PRESCRIPTION DRUGS
The graphs below show the prevalence of prescription drug use disorder by age of first nonmedical use of prescription drugs. Among those who first used a prescription drug nonmedically at age 13, about 42% experienced prescription drug abuse and 25% experienced prescription drug dependence in their lifetime. Note: Before the DSM-V, substance use disorder was divided into classes termed “abuse” and “dependence.” Today substance use disorder is classified as mild, moderate and severe.
Each year that children and young adults delay their first use of any substance, the less likely they will be to develop a substance use disorder later.
Ideas for sharing with others:
Think about your audience. Some people are very compelled by seeing the graphs while others get overwhelmed by the sheer amount of information and tune out. It may be helpful to use one at a time (or only one) and emphasize that for any substance, the rule of early initiation increasing risk of addiction applies.


All Drug Use is Related
Research shows that for teens aged 12-17, all substance use is related.
This means teens that have used any one substance -- alcohol, marijuana, or nicotine -- in the last month are more likely to have used the other two, and other illicit drugs, compared to their peers that have not used any substances. In other words, when parents hear “it’s just a little weed” or “it’s just a little bit of beer” they should be concerned. This pattern holds true for alcohol, marijuana, and nicotine. This is why making One Choice of no use of any substance is best for health.
Click below for more stats




What you should know and how to share it with others

Share the data about how all substance use is related, providing students with graphs and detailed explanations of what these graphs tell them.
Often prevention messaging is specific to individual drugs (e.g., nicotine, prescription drug misuse) or situations (e.g., drunk driving).
The One Choice approach to prevention serves as a foundation on which these more specific prevention messages can be built and/or enhanced.
These are all important and necessary, but for young people all substance use is related.

“”He only uses weed which is safer than alcohol”
“She only drinks at parties, and she’s doing fine at school””

The Fact:
When a teen uses one substance, the likelihood of using a second, third, or more substance increases dramatically.
WHAT THIS MEANS
The following graphs were created from a study, conducted by the Institute for Behavior and Health, using data from the National Survey on Drug Use and Health (17,000 youth aged 12-17 in the US). Overall very few youth who did not use marijuana reported using other substances. By contrast, youth who used any marijuana (even once) were significantly more likely to have used other substances.
YOUTH AGED 12-17 WERE ASKED, “HAVE YOU USED MARIJUANA IN THE PAST MONTH?”
The left half of the slide show is people who DID NOT use any marijuana in the past month. Among youth who DID NOT use marijuana in the past month:
8.0% used alcohol
3.5% engaged in binge drinking
0.4% engaged in heavy alcohol use
2.7% used cigarettes
2.2% used other illicit drugs
The right half of the slide is students who DID use marijuana in the past month. By comparison, among youth who DID use marijuana in the past month:
44.6% used alcohol
27.5% engaged in binge drinking
5.9% engaged in heavy drinking
23.6% used cigarettes
21.7% used other illicit drugs
YOUTH AGED 12-17 WERE ASKED, “HAVE YOU USED CIGARETTES IN THE PAST MONTH?”
The same pattern holds true. Among youth who DID NOT use cigarettes in the past month:
9.5% used alcohol
4.4% engaged in binge drinking
0.6% engaged in heavy alcohol use
5.3% used marijuana
2.7% used other illicit drugs
The right half of the slide is students who DID use cigarettes in the past month. By comparison, among youth who DID use cigarettes in the past month:
39.7% used alcohol
26.7% engaged in binge drinking
5.8% engaged in heavy drinking
36.8% used marijuana
20.7% used other illicit drugs
YOUTH AGED 12-17 WERE ASKED, “HAVE YOU USED ANY ALCOHOL IN THE PAST MONTH?”
The left half of the slide shows those who DID NOT use any alcohol in the past month. Among youth who DID NOT use any alcohol in the past month:
3.5% used marijuana
2.5% used cigarettes
2.2% used other illicit drugs
The right half of the slide shows those who DID use alcohol in the past month. Alcohol use is divided into three categories: some alcohol use, binge alcohol use and heavy alcohol use.
Among youth who DID use some alcohol - but not binge or heavy alcohol use - in the past month:
20.0% used marijuana
9.4% used cigarettes
10.5% used other illicit drugs
Youth who engage in binge and heavy alcohol use were much more likely to have used other substances, underscoring the point that the heavier the use of alcohol, the greater the likelihood of using other substances.

Ideas for sharing with others:
Consider integrating the graphs into your own materials to add compelling visuals about the close correlation between all teen substance use
For Related Materials and Programming Ideas, Click Here
.

More Youth are Making One Choice
There are many misperceptions about the prevalence of teen drug use. Many adults, including parents, teachers, and teens themselves, mistakenly believe that it is inevitable that teens will “experiment” with drugs. The truth is that most young people do not use substances.

While many young people may feel that they are alone in their choice to not use any substances, this is not the case. Data show a growing percentage of American youth are making One Choice not to use any alcohol, nicotine, marijuana, or other drugs. Giving youth who are making One Choice opportunities to share their experiences and reasons for being drug-free can help their peers feel supported and less alone in making One Choice.
Protective Factors Against Adolescent substance use
adapted from Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs and Health.

What you should know and how to share it with others
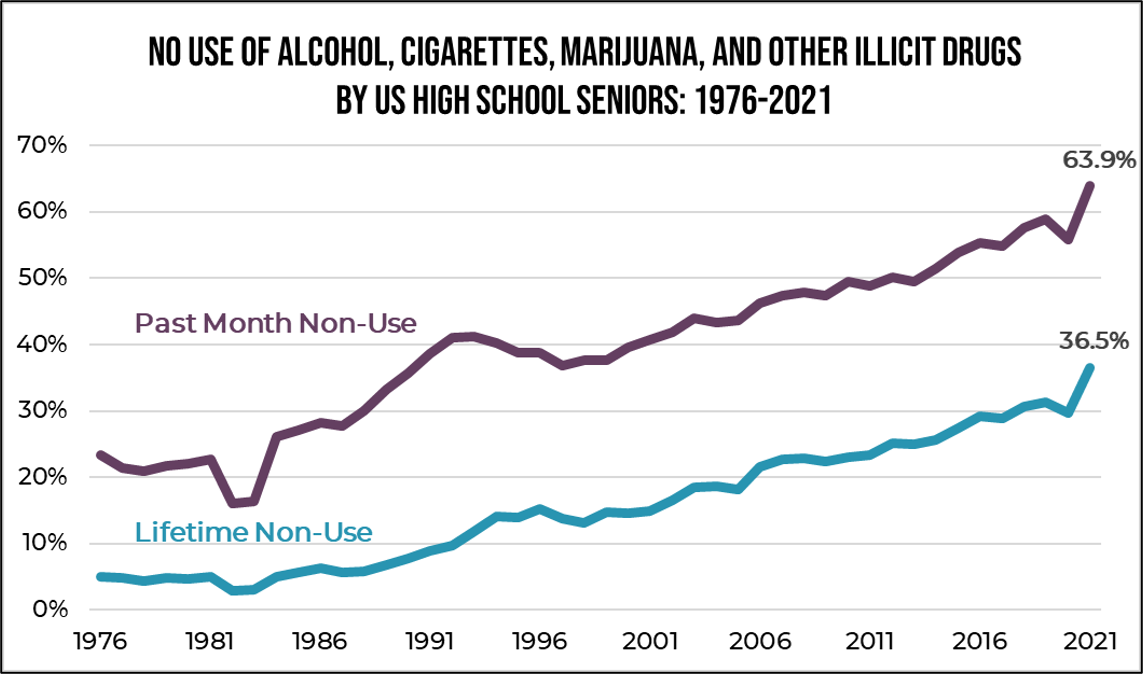
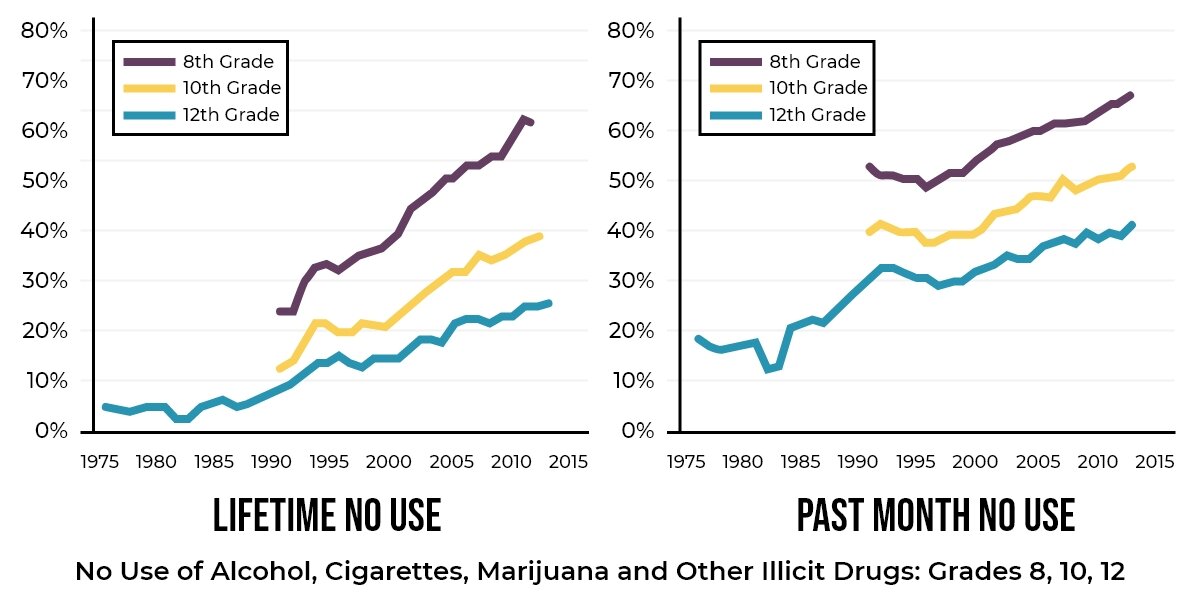
For decades, a growing percentage of American youth have made One Choice to not use any alcohol, cigarettes, marijuana, or other drugs.
Be familiar with your local youth substance use behavior data and find the best ways to promote positive trends in your own community that reinforce that message.
Harness the power of youth-to-youth messaging and youth-to-adult messaging to reinforce that the goal of non-use is realistic.
One Choice is NOT the Just Say No campaign of the late 1980s and early 1990s.
Youth substance use is a health issue, not a moral issue.


Why the One Choice message?
Offers a clear health standard of no-use supported by the science of the developing brain
Supports all other prevention efforts
Promotes teen self-care and autonomy
Provides an opportunity to develop teen leadership
Builds on the trend created by American youth over the past four decades
Anyone and everyone can make One Choice:
Youth who have never used any substance
Youth who may have used in the past but are making One Choice today
Youth with substance use problems actively making One Choice, including those in early and long-term recovery

The fact:
Youth substance use is NOT inevitable.
In 2019…

Far more teens engaged in substance use in the late 1970s and 1980s -- when many parents of today’s teens were young. This is why the trend toward non-use may come as a surprise to so many adults. More than ever, young people are making One Choice not to use ANY substances.
Start a conversation!
Ask youth to find where on the graph their parents would fall as teenagers. How does teen substance use compare to now?
Are there narratives on youth substance use (e.g., “glory days”) that young people hear from adults that contradict their own experiences?
What kinds of narratives on youth substance use are found in media, including films, music, social media?
Invite youth to be part of creating a new narrative based on science and their own experiences.


The Fact:
Marijuana trajectories are a warning that this decades-long trend of no-use may be lost.
Past month substance use by high school seniors 1976-2019, Monitoring the Future
Over the last 20 years, significant declines have been seen in the percentage of youth who use alcohol and cigarettes. Use of illicit drugs other than marijuana has remained relatively low after an initial significant decline in the early 1980s.
After peaking in 1978, marijuana use by youth declined until 1992. Marijuana stands apart from other substances because its use has increased while rates of other substances have decreased.

California’s Proposition 215, the Compassionate Use Act of 1996 - California was the first state to legalize the use of marijuana for medicinal purposes. As of June 2022, 38 states and the District of Columbia have legalized “medical” marijuana and 19 states and the District of Columbia have legalized recreational marijuana.
Who benefits from policies? The marijuana industry spent over $7 million in lobbying the Colorado legislature between 2010-2021 on behalf of policies intended to increase marijuana use.
Start a conversation!
Public health policy has an impact on use:
1984 passage of the National Minimum Drinking Age establishing 21 as the minimum legal purchase age which was tied to annual federal highway funding.
1998 Tobacco Master Settlement Agreement and subsequent massive public health initiative (e.g., Truth campaign) to reduce cigarette smoking.

.

Commercialized Recreational Pharmacology
The global drug problem has been described as commercialized recreational pharmacology, defined as the use of psychoactive drugs that super-stimulate brain reward for pleasure.
This commercial industry, driven by profits, exploits people who use both legal and illegal drugs. Many more drugs (e.g., synthetic drugs), at higher potencies and new delivery systems (e.g., vaping) are being created.
What you should know and how to share it with others

The Fact:
Profits are generated by heavy consumption.
Examples of commercialized recreational pharmacology of legal drugs include the alcohol industry, “Big Tobacco” and increasingly, the legal marijuana industry:
About 80 percent of all alcohol is consumed by only about 20 percent of all alcohol users.
A study from the United Kingdom showed how financially dependent the alcohol industry is on heavy drinkers, producing 68% of its revenue.
Only about 1 in 5 marijuana users engage in daily- or near-daily marijuana use. However, daily- or near-daily use accounts for about 80% of marijuana consumption.
A 2022 study showed that youth who used e-cigarettes in the past month were much more likely to have used marijuana in the past year than youth who did not use e-cigarettes — and importantly, youth who used e-cigarettes and lived in states with legal “recreational” marijuana for adults were dramatically more likely to have used marijuana than youth in states without a legal marijuana industry. “The massive increase in the likelihood of cannabis use among e-cigarette users suggests that state-level recreational cannabis use policy for adults may amplify the individual-level risk factor of e-cigarette use for later cannabis use among youth.”
The marijuana industry spent over $7 million in lobbying the Colorado legislature between 2010-2021 on behalf of policies intended to increase marijuana use.
Minority and economically disadvantaged groups are often targeted by commercial industry; for example:
Research has shown an increased availability of alcohol in predominantly African American communities compared to predominantly White communities.
The Truth Campaign has highlighted the fact that tobacco is a social justice issue with a history of disadvantaged groups being targeted by Big Tobacco.
Will Jones III of SAM (Smart Approaches to Marijuana) authored an op-ed urging against the commercial legalization of marijuana, highlighting predatory practices of the marijuana industry (and others) against communities of color.
Start a conversation!
How is substance use portrayed in the media? Is it glamorized or demonized? Are substances treated differently? What substances are normalized and why?
Have a discussion about the emergence of vaping and related public policy: What kinds of limitations (or lack thereof) are on nicotine content and public use? How has vaping played out in different countries?


How do policies and laws about legal and illegal substances play out across different demographic groups? Are there disparities? How are young people impacted?
In places where marijuana is legal, what has changed and what hasn’t changed? Consider things like: arrests, driving under the influence, youth use, illegal sales/trafficking, tax revenue, etc. One useful resource is from the Rocky Mountain HIDTA which provides an annual report entitled The Legalization of Marijuana in Colorado: The Impact.
What should be prioritized -- public health, profit, individual freedom?
Prevalence of Marijuana Dispensaries in Colorado and Washington State
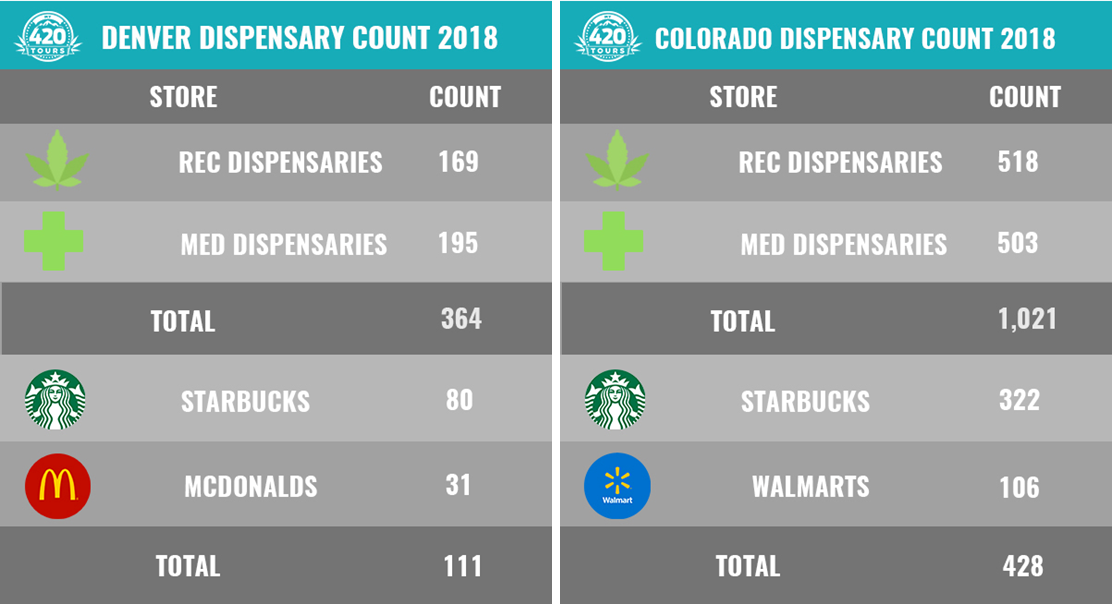
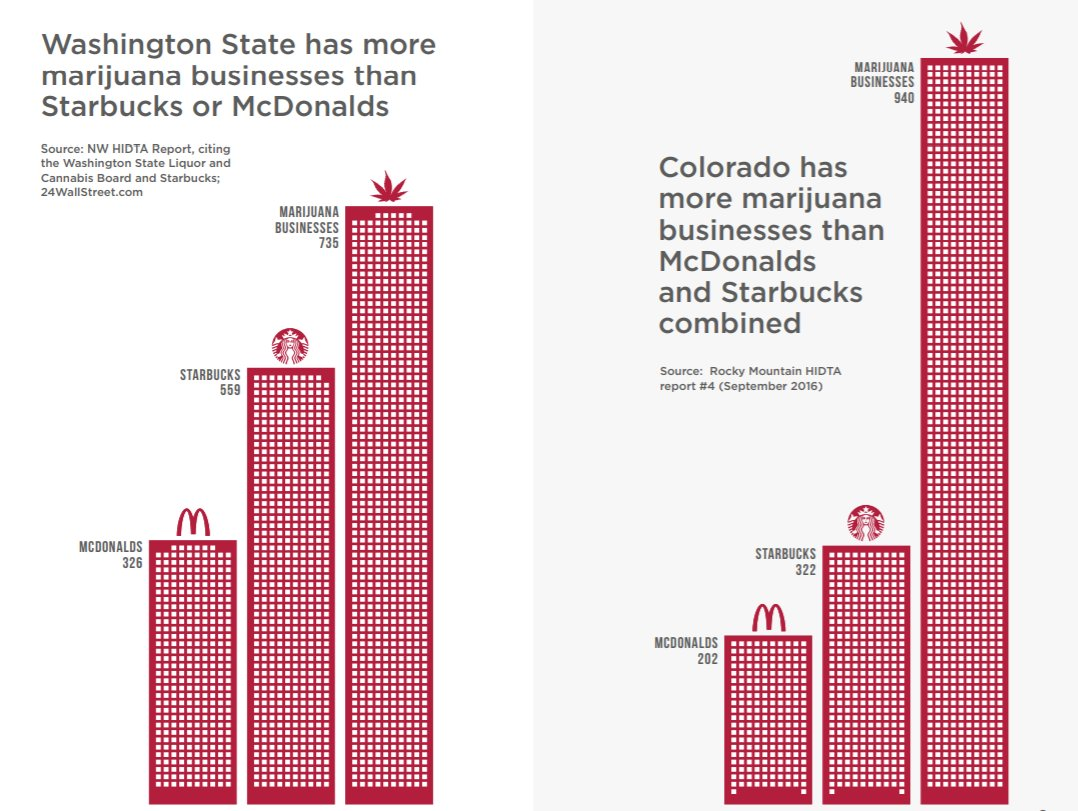
Above graphic comparing Washington and Colorado courtesy of Smart Approaches to Marijuana (SAM).

The fact:
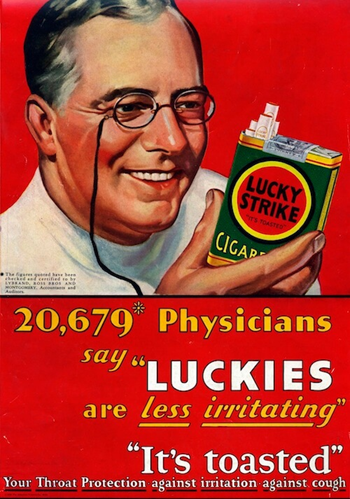
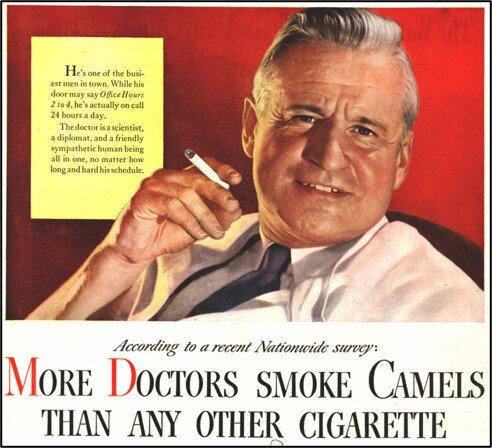
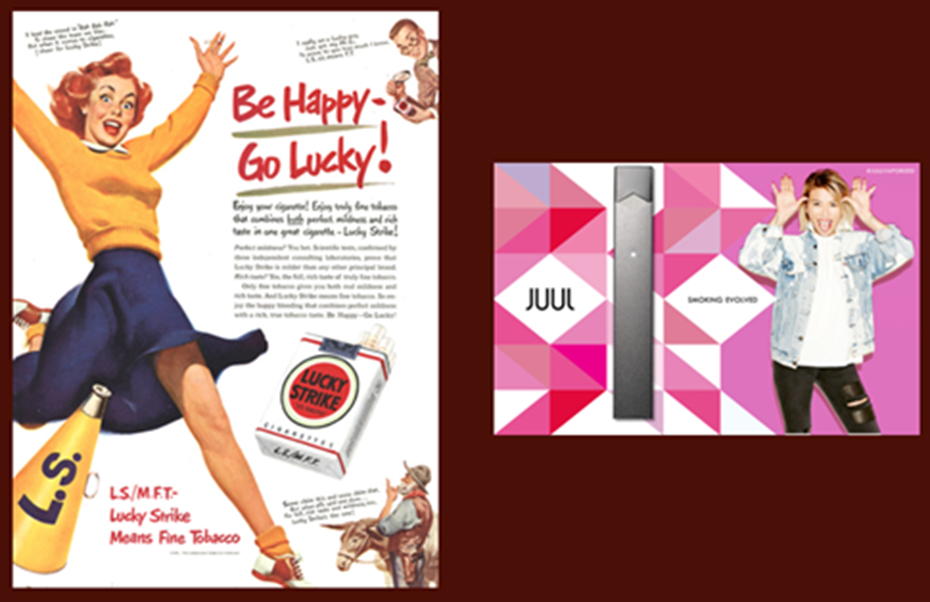
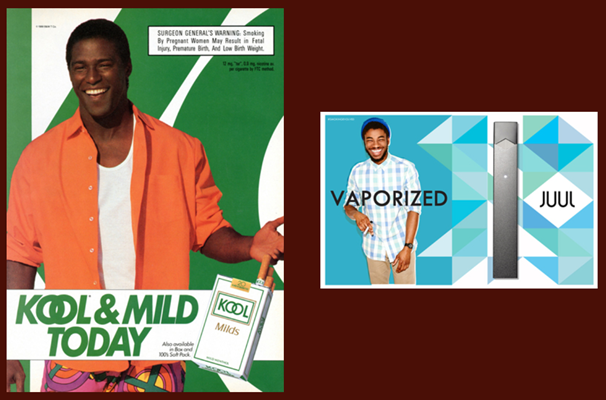
Big Marijuana is using the Big Tobacco playbook
In the past, cigarettes were advertised as safe, healthy, and endorsed by physicians. Now a new industry promotes marijuana as “medicine” and part of personal wellness.
Advertising for commercialized recreational pharmacology ranges across social media and print media, including billboards, normalizing these substances. Consider how many alcohol ads -- and product placements -- you see during a sporting event on TV.


All tobacco and “medical” marijuana ads from Stanford University Research into the Impact of Tobacco Advertising.
“Communities ignore the lessons of tobacco control at their peril. If we’re not more careful in how we regulate legal marijuana we will have a new tobacco-like industry hooking and harming kids with flavors, ultra-potent pot, and aggressive marketing for generations to come.”
“Super Peers”
It is well known that peers are a strong influence for young people. Social media and advertising have been described as a “Super Peer,” with instant access and exposure to seemingly countless “peers.” This has implications for prevention because social media may offer “youth information about substance use that they may not encounter through other channels.” This normalization likely contributes to the glamorization of use and misconceptions such as “everyone is using” and “youth use is inevitable.”

Start a conversation!
Take screenshots or photos of images of commercialized recreational pharmacology seen in daily life as you come across them such as celebrity product placement, advertising on television/sports, among social media influencers, Instagram/Facebook/Snapchat, etc.
What messages are conveyed about health, wellness, safety?
How do companies target young people (for whom the products are illegal)? Consider flavorings, design, social media advertising and influencers.
What kinds of advertising tactics are used by medical and recreational marijuana dispensaries? Compare and contrast to images of the past, e.g., Marlboro Man, Virginia Slims, Joe Camel.
How does “medical marijuana” differ from medicines prescribed by physicians? (Consider FDA-approval - efficacy, safety and consistency of product). What other medicines are “recommended” for use as-needed, as much as you want, for as long as you want?

THE FACT:
Teens are more likely to use marijuana than cigarettes.
Start a conversation!
There is clear public consensus that cigarettes are unhealthy. This isn’t an accident.
Discuss policies that have impacted cigarette use in the country:
Surgeon General’s Report on E-Cigarette Use Among Youth and Young Adults in 2016
Master Settlement Agreement in 1998 which led to massive education campaigns
Passage and enforcement of laws like identification requirements, increased taxes, and tobacco 21 legislation signed into law December 2019
Ask, are there many (or any?) public places where smoking is permitted? Consider changes that have been made to workplaces, restaurants, airplanes, etc.

Discuss policies that have impacted, and continue to impact, marijuana use in the country
“Medical” marijuana laws, recreational marijuana laws
Prominence of shops/dispensaries, advertising, product variety: edibles (candy, brownies, chips, soda), vapes, dabs, waxes, etc.

The Fact:
Vapes are not safe for youth. Vapes or e-cigarettes, a delivery system for nicotine, THC, flavorings, chemicals, and other substances, are a part of commercial recreational pharmacology.
E-cigarette aerosol can contain potentially harmful substances including “heavy metals like lead, volatile organic compounds, and cancer-causing agents.”
E-cigarette companies appear to be using many of the advertising tactics the tobacco industry used to persuade a new generation of young people to use their products. Companies are promoting their products through television and radio advertisements that use celebrities, sexual content, and claims of independence to glamorize these addictive products and make them appealing to young people. —Thomas R. Frieden, MD, MPH, (former) Director, Centers for Disease Control and Prevention, E-Cigarette Use Among Youth and Young Adults A Report of the Surgeon General, 2016
The following images provide side-by-side comparisons of past cigarette advertisements and early ads for Juul e-cigarettes which specifically targeted young users. Images courtesy of Stanford University Research into the Impact of Tobacco Advertising.


youth who vape are more likely to use other substances.
An analysis conducted by the Institute for Behavior and Health of nationally representative Monitoring the Future data showed students who vaped were much more likely to use other substances than their non-vaping peers:
Among 12th graders who vaped in their lifetime, 96% used other substances
Among 12th graders who vaped in the past month, 82% used other substances
.

Substance Use and Mental Health
What you should know and how to share it with others

THE FACT:
Substance use can adversely impact mental health.
People of all ages put their mental health at risk when they engage in nonmedical substance use. The mental health effects of substance use can be brief or can have life-long effects, even after a person stops using. People living with mental health challenges are at higher risk of initiating substance use and at the same time, substance use is associated with higher risk of mental health disorders. Substance use can also worsen the symptoms of an existing mental illness.
Among the shared underlying causes of substance use disorders and mental health disorders are:
genetic vulnerabilities
changes in brain composition
early exposure to trauma and stress, such as Adverse Childhood Experiences (ACEs)


Some of the mental health problems that often co-occur with substance use disorders include depression, anxiety disorders, schizophrenia and personality disorders.
The most common mental illnesses in teens are generalized anxiety, social phobias and depression.


There is no one substance that causes mental health problems. According to the National Institute on Drug Abuse (NIDA), drugs that can cause mental health problems include:
Cocaine • Inhalants
Ketamine • Kratom
LSD • Marijuana
MDMA • Methamphetamine
PCP • Prescription Drugs
Steroids (appearance-and performance-enhancing drugs)
The National Survey on Drug Use and Health found that among the 19.3 million adults aged 18 and older with a substance use disorder, nearly half -- 9.7 million (49.2%) -- also had a co-occurring mental illness.

THE FACT:
Science has shown that high-THC marijuana products can temporarily induce psychiatric symptoms, including those associated with schizophrenia.
A recent study showed daily use of marijuana, particularly high-potency products (more than 10% THC), increased the likelihood of having a psychotic episode later. This is particularly relevant given the dominance of high-THC products in the market, now averaging over 15%.
Start a conversation!
1 in 5 youth will experience a mental health challenge in their life. What mental health are your peers facing?
Where can young people get help when they or a loved one is facing a substance use and/or mental health challenge?
Encourage young people to learn about their own family history and risk factors


Screening for substance use and mental health challenges and providing appropriate intervention can positively change the long-term outcomes for young people. Notably, half of all mental health conditions start by 14 years of age but most cases are undetected and untreated.
There are key roles for individuals who engage with youth in health care settings - primary care, school-based health offices, mental health providers - to provide information about youth substance use prevention and the One Choice message. Prevention leaders, including youth leaders, can engage with healthcare and school sector partners about their role and the importance of screening and early intervention as essential prevention strategies.
.

develop ONE CHOICE initiatives
Here are tips and tools for integrating the One Choice message into your prevention work.
Youth-led campaigns
Engage youth leaders to talk about their concerns about potentially alienating their peers over prevention messages. Youth leaders can assist in creating culturally-sensitive messaging for their peers. Talk about scare tactics -- are they appealing and do they work?
Remember there are a number of factors that play into why young people may engage in substance use. One Choice is not about stigmatizing people who use substances; it is about encouraging and supporting non-use as a health goal for youth.
Consider creating One Choice prevention messages that are for different groups -- students, parents, and the community at large.
I Am One and I Make One Choice Campaign
RyeACT Coalition, Rye, NY
I Am One and I Make One Choice is a message that was created by youth in RyeACT. It celebrates an individual’s non-use by sharing their personal reasons why they make One Choice. It does not pass judgement on another person’s substance use. Students are invited to take a “tile” and fill out why they make One Choice to be drug free.
Download colored tiles for use in your own One Choice initiatives!
Download a sample campaign planning guide for youth leaders campaign planning guide
These tiles can be customized with your organization/group’s logo. Reach out to OneChoice@ibhinc.org and we’ll be ready to help!


I Am One and I Make One Choice
RyeACT’s I Am One Mosaic Wall
RyeACT students also created peer to peer messaging through PSAs:
Shatter the Myths Campaign
RyeACT Coalition, Rye, NY
Rye Middle School and Rye High School worked together to create a “Shatter the Myths” campaign as part of RyeACT’s participation in NIDA’s National Drug and Alcohol Facts Week.


Living the Example Contest
Mentor Foundation USA, Virginia
The Living the Example contest was created to celebrate and empower youth to stay drug-free by providing a powerful platform to speak up and out against drugs and promote healthy living. The contest is organized by Mentor Foundation USA to give young people the opportunity to showcase how they are “living the example” and making a difference in their community.

Peer to Peer MEssaging about Fentanyl
Students in Prince George's County Public Schools in Maryland created a PSA in English and Spanish to warn their peers about fenanyl.
Parenting & Community Education Resources
Reach out to OneChoice@ibhinc.org for assistance in adapting any of these resources for your local community.
ONE CHOICE PARENT EDUCATION TRI-FOLD
IBH and RyeACT teamed up to create an educational tri-fold for organizations interested in sharing the data behind One Choice with parents and caring adults working with youth. This tri-fold, available in printable and digital formats, can be customized for your needs with local data and your logo:
PRINTABLE TRI-FOLD DIGITAL TRI-FOLD


THE ONE CHOICE 5
Five key points that parents and caring adults should understand about prevention:
Youth Substance Use is NOT Inevitable
Be Brain Development Savvy
Be Substance Savvy
Talk Early and Often
Act Quickly If You Suspect Substance Use

English

Spanish
WHAT DOES IT MEAN TO MODEL HEALTHY BEHAVIORS?
What do you do in moments of stress, joy, and sociability? If your responses always or often include alcohol, marijuana/THC, or other substance use, add responses that do not include substances to model alternative strategies for your kids

PARENTING FOR PREVENTION 101 CAMPAIGN
The RyeACT Coalition developed a parent-focused prevention campaign kicked off with a Parent University event. A series of handouts on development from childhood to early adulthood were developed and can be adapted for other prevention group’s parent-focused initiatives.
Download the Parent University handouts by student age:
CHILDHOOD GRADES K-3 , MIDDLE CHILDHOOD GRADES 4-5, PRE-ADOLESCENCE GRADES 6-8, ADOLESCENCE GRADES 9-11, EARLY ADULTHOOD GRADE 12+ ALL AGES


Like what you see? Support Our Work!
Support the One Choice prevention initiative of the Institute for Behavior and Health, Inc., a 501(c)3 non-profit organization, with a tax-deductible donation.
Tips for adult leaders working with youth
SEEK THEM OUT & INVITE THEM IN:
Remember that EVERYONE can make One Choice... so when looking to engage young people in prevention activities, cast as wide a net as possible; encourage ALL youth who are interested to get involved—not just those who identify as “lifetime non-users.” Sometimes getting involved is the first step toward making One Choice.
Think about ways to engage youth leaders in other youth organizations/clubs/ groups that have interests that overlap to collaborate on initiatives, campaigns, or events.
Examples might include:
Those interested in youth mental health or suicide prevention
Those who work on public policy advocacy or civic engagement (civic clubs)
Those interested in LGBTQIA+ issues
Those who advocate for disabilities or special needs
Those who care about environmental issues

Enlist youth leaders to recruit peers who might want to get involved – one of the easiest and most successful strategies is the “Bring a Friend” approach; encourage your student leaders to “bring a friend”...no commitment required, just come to a meeting or an event; many stay involved (as long as your meetings are meaningful and fun!)
Work with schools and other community organizations (coalition partners) that have youth groups to collaborate on events and projects of mutual interest; this is a great way to increase visibility and “find” youth leaders.
Actively seek a diverse group of leaders that reflect the diversity of your community and a wide range of interests, groups, and grade levels (some age groups may require separate groups).
Create opportunities for All the youth leaders you get—be sure to build in “behind the scenes” and “front and center” opportunities to accommodate all types of leaders. Great teams need ALL kinds of leaders. Great adult advisors know how to incorporate all voices.
INVEST in Them & INVEST in Their Ideas:


Provide tools and resources, leadership development and skills training to ensure your youth leaders have what they need to carry out initiatives and messaging campaigns with confidence and success.
Connect with other groups and organizations in your community that care about youth leadership development; they may have things to “give” – talent and skills to teach, connections to make, access to decision makers, budget dollars to support youth training or event sponsorship, etc.
Ask for their input and ideas and find ways to use them; dedicate funds and resources to bring their ideas to fruition; be open to having them change your mind – and know when you might need to provide perspective or information to help change theirs.
Give them the chance to lead, but not without first providing the tools and skills to succeed (provide training, networking opportunities with other youth leaders such as the OCC, CADCA Youth Leadership Initiative, Youth to Youth conferences, other local and regional youth programs).
Find out what matters to them...and then make sure it matters to YOU and other adult community leaders.
Give them opportunities to shine and celebrate their hard work – including, most importantly, their decision to be drug-free (community presentations, features in the newspaper and TV ads, recognition programs at school in the community, highlight them in your newsletters, etc.)
Don’t ask them to do more than you are willing to do yourself.
Make it Work for THEM and DON’T FORGET THE FUN!
![iStock-1218950556-[Converted].png](https://images.squarespace-cdn.com/content/v1/58b590e5c534a5d38a84f013/1624038719917-3VZ5EO5JIEUUD6QZ63DO/iStock-1218950556-%5BConverted%5D.png)
Young people often have many things “competing” for their time; they tend to stick with the ones that are meaningful, that include a clear benefit for them, and the ones that are FUN!!
Be flexible with meetings so you can meet at times that work for their busy schedules; 9 times out of 10, YOU will need to bend for them...not the other way around.
To the extent possible, try to have “the work” (planning, prep work, etc.) happen within the confines of your meeting times – they already have demands of homework, family obligations, other extra-curricular activities, and sometimes jobs – they don’t need more “homework”.
Work to have a big enough “bench” so that no one person (or small group) has to do all the work; this also helps when schedules get busy (i.e., if someone is busy in one season with school or a sport or activity, but then has more time later).
Meet in places that are easy for young people to access: meet in school buildings after school, meet in community locations that are accessible on foot OR via public transportation as much as possible.
Don’t forget “WIIFM” (aka “What’s In It For Me?”). Engagement is a two-way street; they are giving you their time, their talents, their ideas, and their power to influence their peers. What are YOU giving them in return? Make sure it’s something they actually want/need. Connection to like-minded peers, a safe place to have drug-free fun, connection to an issue that matters to them (and power to effect change around that issue), community service and leadership opportunities, etc.

Incorporate FUN...meetings, events, and initiatives that include games, activities, music, dancing, food, etc.
Be sure to acknowledge and recognize their efforts in the community and beyond. The decision to speak out about being drug-free as a young person in our current times is, in and of itself, an act of bravery. Acknowledge it. Celebrate it. Get community leaders to recognize it. When you do, more youth will follow....because everyone wants to be part of something that makes them feel special and valued for who they are!
Tips for analyzing local youth substance use data
How can we learn if the youth in our community use substances at the same rates and in the same combinations as reported in national youth surveys? How can we learn if youth in our community make One Choice?
IDENTIFY available Data Sources
Many schools administer self-report student surveys on substance use and other health behaviors. The surveys conducted may be part of larger national studies such as the Youth Risk Behavior Surveillance System (YRBSS) and Pride Surveys, or state-based surveys such as the California Healthy Kids Survey, Tennessee Together Student Survey, and Florida Youth Substance Abuse Survey, etc.
Evaluators who work with prevention organizations may be able to assist in locating and analyzing youth substance use data collected in your community or state. They will need datasets that contain individual-level data.


Identify DATA ELEMENTS
Demographics
Essential demographics include:
grade/age • sex
race/ethnicity
Substances
Determine whether youth (however “youth” is defined) have either used or not used (yes/no) the following substances in the past month and/or in the past year:
alcohol • vaped • cannabis/marijuana
cigarettes/tobacco • other illicit drugs
If available, consider adding other substance use variables (e.g., binge drinking, nonmedical use of prescription drugs) and frequency of use.
ANALYSES
Substance Use
By coding past month (or past year) use of a particular substance as Yes=1 and No=0, an evaluator can calculate the number and percentage of students who used each substance.
A series of cross tabulations could identity the percentage of students who used each one of the substances and who also used each of the other substances. These could be further broken down by grade, age, sex, etc.
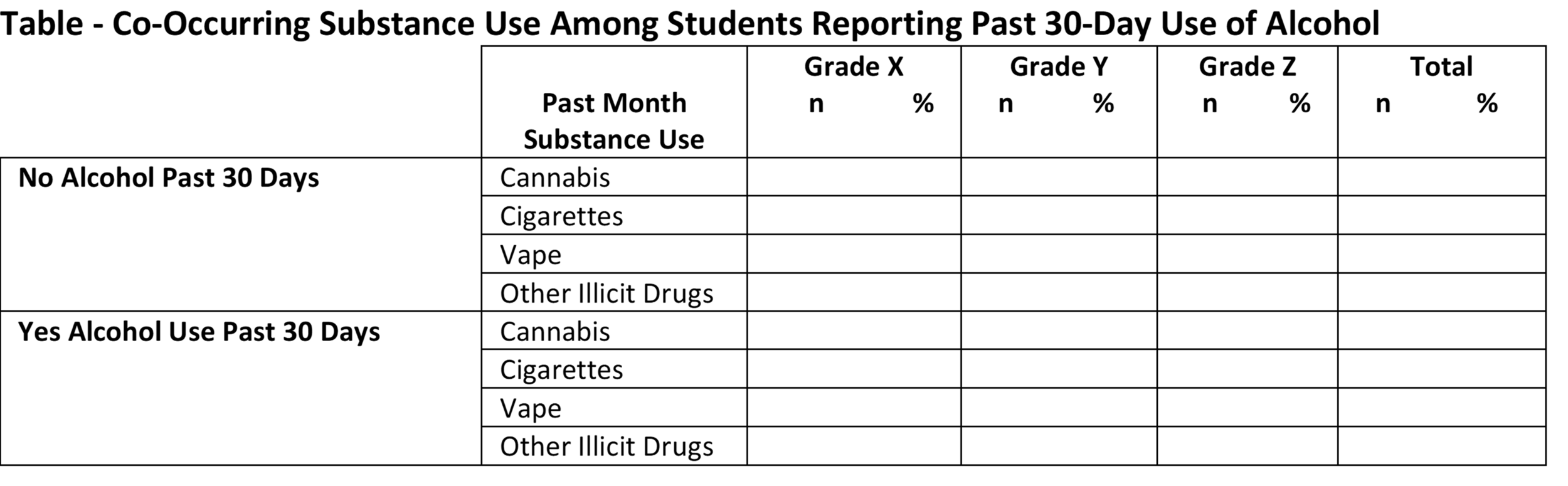
Other tables to follow would include:
Co-Occurring Substance Use Among Students Reporting Past 30-Day Use of Cannabis
Co-Occurring Substance Use Among Students Reporting Past 30-Day Use of Cigarettes
Co-Occurring Substance Use Among Students Reporting Past 30-Day Use of Vaping
Co-Occurring Substance Use Among Students Reporting Past 30-Day Use of Other Illicit Drugs


Substance Non-Use (One Choice)
Calculate and report the overall percentage of students who did NOT use any substances: By summing the 1s and 0s across the 5 substance categories for each student, an evaluator can identify those who have made the One Choice of non-use (sum=0). Break this group down by the relevant demographic subgroups.

The evaluator can use the same method to identify youths who used a single substance (sum=1) and polysubstance users (substance use total is >1).
TIPS FOR REPORTING
· When generating tables and graphs, make sure the overall sample sizes are listed.
· Be clear what the denominator is in each table.

COMPARING LOCAL DATA TO STATE DATA
The National Survey on Drug Use and Health (NSDUH) provides data for the nation and state-by-state that can be used to compare to local community data.
NSDUH provides an interactive map with state and sub-state substance use levels for alcohol, cigarettes/tobacco, and marijuana (cannabis). Although the map and graphs that can be generated on the site only show use for “individuals aged 12 or older,” evaluators can click on the CSV icon to download an Excel file that has the data for various age groups, including ages 12-17. Such data can assist with checking the validity of findings for these three drugs.
Engaging Parents and Families
Consider creating One Choice prevention messages that are for different groups including parents and families — and the community at large.
Parenting for Prevention 101 Campaign
RyeACT Coalition, Rye, NY
RyeACT developed a parent-focused prevention campaign kicked off with a Parent University event. A series of handouts on development from childhood to early adulthood were developed and can be adapted for other prevention group’s parent-focused initiatives.
Download the Parent University handouts by student age: Childhood Grades K-3, Middle Childhood Grades 4-5, Pre-Adolescence Grades 6-8, Adolescence Grades 9-11, Early Adulthood Grade 12+


Parent Pledges
Some groups have used parent pledges in their efforts to educate parents on their essential role in preventing youth substance use including SafeLaunch in Santa Barbara, CA and Parents 2.0 Movement, a national campaign.



.
THE ONE CHOICE COMMUNITY
The OCC is a collection of prevention organizations, coalitions and individual leaders who have integrated the One Choice prevention message into their own prevention initiatives.
Join the One Choice Community today!
Learn more about members of the OCC.